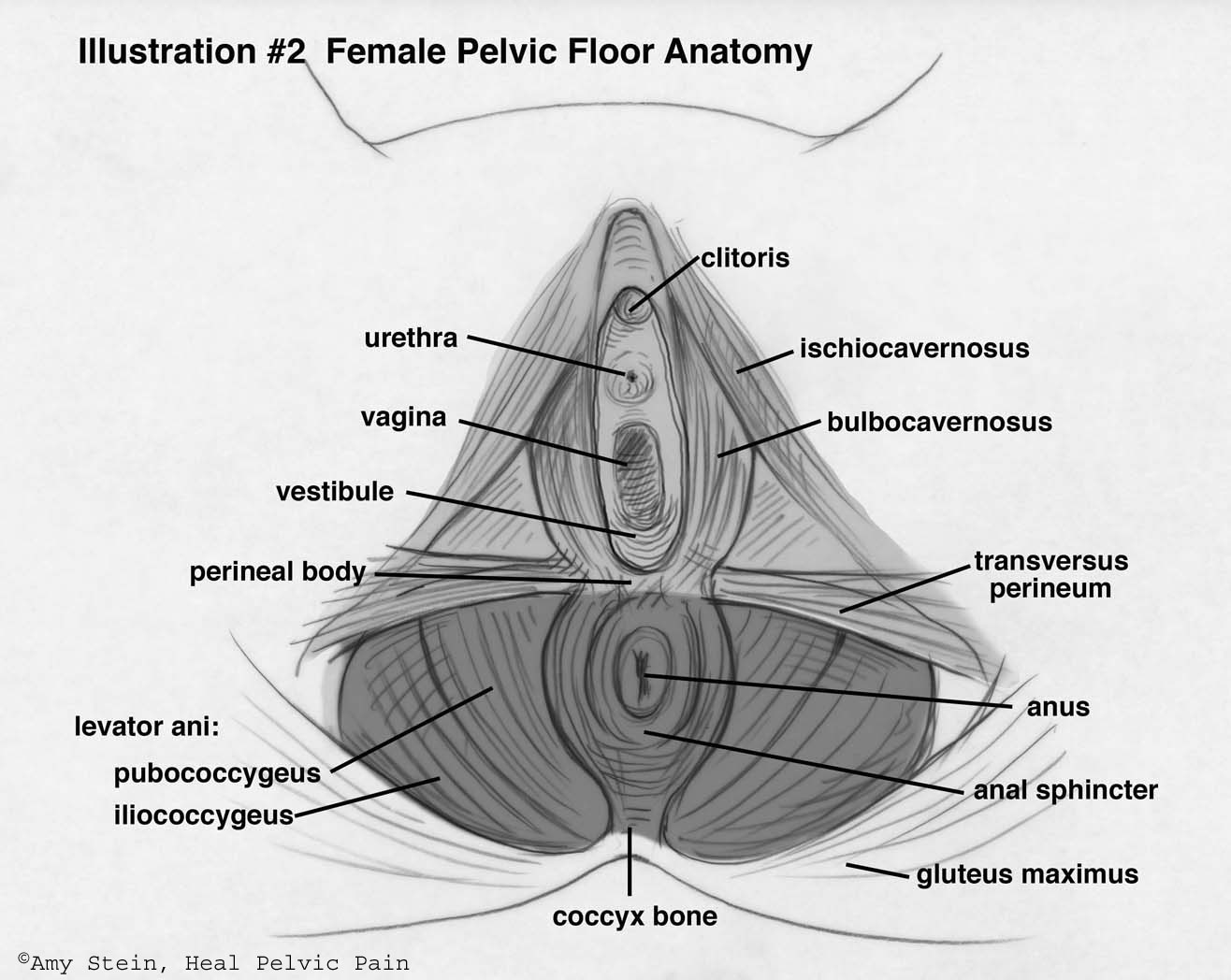
Many evidence based studies prove that pelvic floor physical therapy is an effective treatment approach for men and women suffering from pelvic pain caused by tight muscles and restricted tissues. The pelvic floor muscles, namely the levator ani, coccygeus and obturator internus can develop adhesions, tension or trigger points which restrict movement and cause pain. Trigger points are palpable spasms/knots within muscle tissue and can occur in pelvic floor muscles. Trigger points can lead to adhesions of fascia/connective tissue of the abdomen, groin, pelvic floor and even restrict the viscera (colon, uterus, bladder, prostate gland) within the pelvic bowl.
The pudendal nerves and its branches, traveling from the sacrum (back of the pelvis) and running all through the pelvic floor region innervates the vaginal/penile and rectal areas. The nerves can become squeezed as it travels through tight muscles and fascia, which then decreases optimum pelvic floor function and increases pain.
The pelvic floor muscles are located INSIDE our bodies, in women the muscles are approximately 1-2 inches up from the vaginal/rectal region and in men, the muscles are approximately 1-2 inches up from the base of the penis/rectal region.
The pelvic floor muscles are key for four functions of the body:
1) lower back/core stabilization; 2) normal urinary function; 3) good bowel function; 4) satisfying sexual function.
As a core stabilizer, the pelvic floor works with 3 other core muscles, the Transversus Abdominus (deepest stomach muscle), Multifidus- (deep low back extensor muscle), and deep fibers of the Iliopsoas (hip flexor muscle). These 4 muscles work together to keep our core strong, flexible and prevents lower back pain. If one of the 4 core stabilizer muscles becomes weak or injured, then the other 3 muscles have to work harder to compensate. Over time this puts great strain on the whole core, which leads to back pain/stiffness/weakness.
The pelvic floor muscles are directly involved with three bodily functions, urinary, bowel and sexual.
For functional urination, the pelvic floor muscles surround the urethral opening and should relax when you are voiding and maintain closure or tension when you are not voiding. If the muscles are in spasm, urinary symptoms such as leaking, or feeling a strong urge to void, or having to go to the bathroom multiple times a day (called urinary frequency) and/or being awoken at night to void more than once (called nocturia), can occur. Women using public restrooms should not “hover” over the toilet, as this sustained half squat creates tension in the pelvis and does not allow full relaxation of the sphincters around the urethra to allow full urination. Best to use the protective toilet seat covers and sit comfortably.
For normal bowel movements, the pelvic floor muscles should be able to open and widen to allow the full passage of stool. When not having a BM, the pelvic floor maintains tension at the rectal opening to prevent leakage. If the pelvic floor is weak, leakage can occur. If the pelvic floor is tight, constipation resulting in sitting too long at the toilet, straining to defecate can occur. Toileting should take no longer than 5 minutes following the urge to void. Even though you may not feel completely empty, it’s better to stand and leave the bathroom versus continue to sit and strain. Constant straining can result in hemorrhoids and/or the development of a rectocele, which further impedes good function.
For satisfying sexual function, the toned and flexible pelvic floor allows for more intense orgasms in men and women. A fully relaxed pelvic floor helps women experience pain free intercourse with their male partners. Many patients who are experiencing sexual pain may experience difficulty with partner relationships or even avoid them due feeling of shame or inadequacy.
Pelvic pain due to restricted muscles can be released and return to normal function, no matter how long a person has been experiencing symptoms.
Physical therapists trained and mentored in pelvic floor work can:
- apply targeted manual therapies to rid muscles of trigger points
- utilize biofeedback therapy to help patients learn how to either downtrain (relax) their pelvic floor or to uptrain (strengthen) the pelvic floor
- perform visceral mobilization to improve the mobility of organs lying within the pelvic bowl
- mobilize and teach a patient self-connective tissue (skin rolling) techniques to abolish tight skin and fascia of the inner thighs and abdomen
- teach patients gentle stretching techniques with foam rollers, tennis balls, knobbles, Theracane, S –wands and dilators
- educate in exercises for a strong core
- teach diaphragmatic breathing and visualization to help lower tension of the pelvis and to increase oxygenation to the body and decreased stress
- guidance in cardiovascular exercise to pump more oxygen and nutrients to the tissues
- teach proper bladder and bowel techniques and habits
Most people start to feel better after 2 months of consistent, twice a week therapy which incorporates many of the above techniques. Some reach goals sooner; others may take up to 3 months. By attending regular pelvic floor physical therapy and performing all the home exercises, faulty pattern are reversed and many people are pain free within 2-3 months.