Hypertonus of the pelvic floor is extremely common and often treated incorrectly (as general pelvic floor weakness) because many do not understand the biomechanical functions of muscle well. The problem lies here:
1. There is some sort of pelvic floor or low back or hip issue.
2. The pelvic floor is evaluated for “strength” because it is well understood that in order to maintain correct skeletal orientation and pressures on nerves and ligaments and stuff, the pelvic floor is really important.
3. The pelvic floor evaluation comes back as NOT CONTRACTING WELL, as measured by EMG (electromyograph) or by good old fashioned pressure on a finger.
4. The low-force producing pelvic floor is deemed weak and one is typically given strengthening exercises.
This is all very logical, but unfortunately the very large oversight is that tight or hypertonic pelvic floor muscle will register as “weak” because it is unable to generate force due to the fact that this muscle is already in its tightest (and shortest) position.
Currently there is no agreed-upon clinical standard for measurement (i.e. value of EMG or the finger test) that indicates, when the pelvic floor is not performing correctly, if it’s because it is too tight (read: short) or too loose (read: long). The general misunderstanding seems to be that all a weak muscle needs is a little EXERCISE to fix it up. In actuality, research shows that MORE KEGELS, MORE CORE TENSION, AND MORE SUCKING IN THE GUT MAKE THIS PROBLEM WORSE AND NOT BETTER.
Most pelvic floor issues are created not by one-time events like pregnancy or a skiing accident (like falling on a hip), but by habits that accumulate over time — especially those habits we all share — sitting in chairs the bulk of every day, not using a squat throughout a lifetime, exposure to chronic stress, and then, of course, doing extreme correctives and overdeveloping tension in the abdomen and pelvic floor.
This is a letter from my inbox, which the author gave me permission to share with ya’ll:
Dear Katy,
I was hoping the Pelvic Floor Guru in you would have some pearls of wisdom for me. I am 35, a virgin (sad as that may be, it’s not my main problem!), and have a steel trap for a pelvic floor–not in a good way. There have been times when a pap smear/etc. were in order, but no doctor has been able to get a speculum in. Not even an “infant” size. The smallest of tampons is uncomfortable. You can imagine the implications this has on my life.
If you think of the vagina like a clock, 3 and 9 o’clock (hip to hip) seem fine, but there is NO give at 12 and 6 (front to back). Does that make sense?
I have several of your DVDs and do the “Down There” stretches every day. I’ve talked to a RN, who is also a physical therapist specializing in the female zone, and she says there are some things she could try to help get those muscles to unclench, but, frankly, it sounds the opposite of delightful.
Boy-howdy, do I hope you have some ideas for me! Thank you for any thoughts you may have!
First of all, thank you for writing, lovely reader. Your description of front-to-back tension is very clear — thank you for that. When you have tension in this direction, it is key to learn about the sacrum and how the pelvic floor can act upon it (read more here) as well as understand that the butt muscles are strong force generators that should be keeping the PF muscles supple in the front-to-back direction.
Understanding the roll of the bum to keep the pelvic floor healthy, full-of-blood (not in a vampire/Halloween way, but in a “hey, I’m healthy, used, and full-of-blood kind of way”), and to provide appropriate leverage for the pelvic floor is essential.
No butt, no pelvic floor. Know butt, know pelvic floor.
Someone should make that a bumper sticker. You’d put that on your car’s rear end, yeah?
Anyhow. When hypertonus is diagnosed correctly, there’s usually one option when it comes to what your insurance will cover and that is physical therapy, but most specifically, “internal work.”Internal as in
Checking your oil.
Going under the hood.
Gettin’ one’s hands dirty.
And, a bunch of other euphemisms that seem to relate to cars.

P.S. Isn’t this a great book cover? I just found it on Amazon (click) and think a Do-It-Herself Guide a great graduation gift for any women heading off to the next steps in life!
So, what’s the problem with internal work? Well, if your pelvic floor has developed some sort of chronic issue that is causing you grief, chances you, like the writer of the email, are not very enthralled with the idea of some stranger poking around in your goods.
Because I am the Queen of Down Under,

I will attempt to shed a bit of light on both the process of internal work, my personal experience with it, as well as things you can do that can also improve hypertonus if you’re not ready to get down with your bad self. To help me out, I’ve brought in Pelvic Floor Physical Therapist Susan McLaughlin.
Susan is not only a bad-ass therapist, she’s also a graduate and Master-Teacher-in-Training of our Restorative Exercise™ Whole-Body Alignment program. She does internal work a lot, so I’m going to have her explain what the process is “like” for those who want to know.
So, Susan. Is internal work as creepy as it sounds?
There is a lot of taboo in our culture about genitalia, incontinence and sex and so first of all, it can be an uncomfortable experience to share your pelvic floor issue with your friends or even health care provider. Don’t let that stop you, please! For me, as a practitioner, internal work is a key component to understanding the state and function of the muscles, fascia, potential scar tissue and nerves. So, no, not creepy.
I don’t know, Susan. The word “genitalia” is kind of creepy. But then again, so is the word “creepy,” so I might just be overreacting.
Can you explain a bit about the actual process of internal work? Once when I was getting a facial, I was all relaxed and my face was warm and wet and I had a small fluffy animal placed over my eyes to really make it a spa-like, relaxing experience you know? Then, out of the blue, I hear this sound like someone is being electrocuted, and then I realize that the buzzing and zapping electricity thing is now touching my face, which is wet and my eyes are covered… I had a major freak out that ruined the facial. Even though the therapist knew that the electrical-zappy thing wouldn’t hurt me, I didn’t.
Wow, that was a long story.
But important! Because I, like most people, don’t like to be startled in a session, so I want to know everything that’s going to happen. What is a session with internal work like?
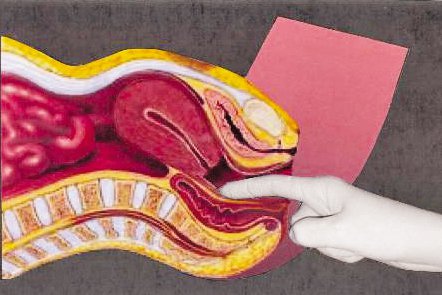
Prior to the internal exam, a superficial assessment is performed.
Sorry to interrupt. Just wanted to clarify that a superficial assessment does not in anyway imply that the practitioner is a shallow person, but that before going in, they take a look around at the surface. You many continue.
The practitioner visually inspects the skin (identifying redness due to inflammation, discoloration, swelling, etc) and observes the perineum for tissue integrity/responsiveness during a pelvic floor contraction, cough and bearing down, as well as palpation of the superficial muscle for tenderness, symmetry. The internal exam is a one finger vaginal (or rectal) assessment. The client is asked to perform a pelvic floor contraction. The quality and strength of the contraction is assessed as well as the ability to return to resting position. If a person is not in a painful state, it is good to assess the endurance of the muscle by having the person hold a pelvic contraction for 10 seconds and then repeat as many repetitions as they can until they fatigue. Quick contractions are assessed by having the client repeat as many as they can in 10 seconds. Again the quality of the muscle activity is important. Some people contract, but never go back to resting position…that is not good. Also the muscles are palpated for tone, tenderness, trigger points. The process is then repeated on the other side.
You sound smart and all clinically and stuff. Do you wear a white coat while you do this?
A lab coat is not my style, though many PTs wear them.
Well, so far it sounds swell. Like a massage, only not ![]() But this is what everyone really wants to know: Does it hurt?
But this is what everyone really wants to know: Does it hurt?
Initially, the evaluation and some follow-up visits may be painful. As the muscles and fascia begin to release, the holding patterns let go and many people experience pain relief during the internal work.
As a biomechanist, I’d like to chime in here for a second about the pain thing. Knowing how sensory receptors work and having had internal work myself, would you agree that the amount of pain felt is equal to the amount of tension or resistance to the pressure being applied? Meaning, the therapist might not be pushing at all, it’s the muscles pushing BACK that cause pain. And if one could use the pain as a mental signal — “oh, here is a place that needs to soften” — instead of just thinking — “Damn Woman, stop hurting me!”, wouldn’t the sensation of “pain” instantly lessen?
Yes, actually. I have people practice breathing and mindfully letting the muscles go. I can feel the change in the muscle instantaneously if they are able to do that… and most people can.
Ok. So you’re really just helping people become aware of tension patterns they didn’t even know they had, and open their eyes to a situation that they can actually fix themselves! With a little help, of course…
How does an internal work session compare to a Pap exam? This one time, I thought I’d schedule my annual Pap on my birthday. Which, I just wanted to let everyone know, is not as good of an idea as it sounds. But anyhow, please continue. I just thought you might be interested in knowing the highlights of my Pap history.
Thanks. The sessions are different than a Pap because there is no speculum used. And internal sessions are focused on the re-education of muscles, habits, movements, alignment. If a person is experiencing pain, it is important to teach them how to relax the pelvic muscles. Because these muscle have been held in tension it can be difficult to know how to relax. I have found it very helpful to use a finger inserted at the vaginal opening to assist with the cue to “drop” the pelvic muscle downward/backward. A slight pressure onto the muscle provides stimulus to tell the muscle to let go. This can be helpful for the first few visits until the person has confidence in performing the relaxation on their own. Each therapist has their own manual therapy skills to assist in releasing the muscle/fascia/joint dysfunction.
It sounds very clinical and not that fun. Do you ever laugh at all? I mean, not tell dumb jokes or anything (like me), but would you recommend we pick a therapist they feel comfortable with? To me, a therapist is like a pair of shoes in the store. If they don’t quite fit in the beginning, does the relationship improve? Or, better yet, do people have the right to “interview” an internal therapist for maybe 5 minutes to see if they feel relaxed in general? What are your thoughts?
I am being very clinical right now, my bad. I do actually have a sense of humor and am able to help people feel at ease. I like to explain to people what I will be doing so people know what it going to happen and they can choose whether they feel comfortable or not. Comfort is a big deal. It’s a good idea to call a clinic before you make an appointment and have a quick chat with the therapist to see if it would be a good fit.
Ha ha. You said make sure your vagina therapist is a good fit. Get it? (P.S. If you didn’t laugh at that, then pause, take a breath or two, and see if you can relax your pelvic floor muscles Right Now and read it again!)
Anyways. Do you use equipment? Wires? Electrodes? Headlamps?
Currently I don’t use any equipment. However, many therapists utilize biofeedback, electrical stimulation or TENS.
Oh, right. A TENS. Um, do you want to tell us what a TENS is?
A TENS unit (transcutaneous electrical nerve stimulation) is something that clients can use at home for pain. There are external electrodes that stick to your sacral/low back area or on your abdomen. The electric impulses travel through the nerves to the spinal cord and block the pain impulses that go to the brain (basically keeping the secretary busy so she can’t relay the message to the boss that something is going on). This doesn’t hurt and can actually allow some temporary pain relief. You can buy them off of Amazon for like 40 bucks.
Thanks for explaining the TENS. Although I think many people find a nightly glass or two of wine to be effective ![]()
Ok, back to internal therapy. How long does it take to work?
Generally, it may take anywhere from 6-8 visits. Of course, this depends on many factors: is the client doing their home play, how long they have experienced the issue, etc.
Ok. So how does internal work work. (Seems like a lot of work.) Are you fixing my muscles for me? What am I supposed to do/feel/change?
Physical therapy can help facilitate joint mobility and release of fascia and muscle trigger points. The client should begin to become more aware of the pelvic floor muscles as well as all muscles. Notice habits like holding breath, sucking in, excessive sitting and begin changing dysfunctional patterns. The key to lasting change is held by the client. In all of my sessions I emphasize whole-body alignment principles, stress reduction/management, exercise and movement, and nutrition when appropriate.
Is there homework?
Always homework! Restorative Exercise™ and every-day alignment principles.
I’d like to jump in and offer my favorite, get-the-heck-off-your-sacrum, you are damaging your pelvic floor tip here — make sure you are sitting in neutral pelvis and not on a slightly tucked one.
What’s internal work like for a practitioner? What are you feeling for?
The practitioner is feeling for muscle tone/twitch, connective tissue mobility, dense thickened bands in the tissue, adhesion, and symmetry between sides.
Most people think of pelvic floor as just the vaj, but after my vaginal delivery, I developed a hematoma that burst and it seemed to send my deep hip rotator on that side into a spasm. No amount of stretching or specific correctives could get to it and I could still feel that something was off in my hips, even though my vaj was fine. During my session, through help in “finding” the tension I was carrying, I was able to let go of the protective mode I’d been in for almost a year. It made me cry, and not because it hurt. It didn’t! But I just had all this feelings — tense, sad, worried, joy, relief — tied up with this one tiny spot and the event of my son’s birth and, who knows what else! Do other people cry or do seemingly unrelated things?
One of our deep hip rotator muscles called the obturator internus can be palpated and accessed easily through the vagina. This muscle can be a key site in pelvic pain syndromes due to the close connection with the pudendal nerve. The pudendal nerve is the nerve to the muscles of the pelvic floor. Its course of travel runs right over this hip rotator muscle. Tension in the hip rotators can cause irritation of the nerve, and then pain.
And the crying?
Candace Pert, MD was the first to scientifically prove the biochemical basis of emotions. And these emotions, she found are neuropeptides residing not just in the limbic system, but flow throughout the whole body in the nervous, musculoskeletal, immune and cardiovascular systems.
You experienced an emotional release through the fascial and muscle memory! It’s cool stuff and I witness this in my office on a regular basis. This is normal and very liberating. I applaud anyone who is able to feel safe enough to let the emotional release happen.
Word.
So Susan, tell me. How did you get into vaginas? I mean pelvic floor health?
I landed a job as a spine specialist and they asked me if I had any interest in women’s health and I said “Hell Yes!” I started taking courses toward my specialization. When I was an anatomy teacher’s assistant I had a fascination with the sacrum. I felt that it was a powerful bone and I felt that, because the pelvis is the area of our center of mass, that there has to be a lot going on in there. Also, my favorite color is orange, the color of the second chakra, the pelvic area…my fate was set!
Orange is your favorite color? Mine too! I never thought about it like that, although I’ve been fascinated by the pelvis ever since taking anatomy as an undergraduate. Do you think or natural interest in orange pelvises and vaginas is why we get along so well?
That and our high sense of fashion! <—— This is a very funny joke that is probably only funny if you spent a week going through our similar wardrobes of sweats, track pants, yoga pants, and fancy yoga pants for formal occasions.
What do you love the most about women’s health work? What do you wish more people understood about their pelves?
I love that the pelvis is our center. It is the house of our womb and bowels. I would like women and men to feel more comfortable expressing themselves to healthcare workers and friends, so pain and dysfunction doesn’t go on for years.
Also, I wish people understood that their daily habits and movement patterns contribute to pelvic pain and that there is a way out of pain without meds and surgery, through awareness and movement.
I really love that. The solution to chronic pain — pelvic, in this case, but of course, it’s the same for all tissues — is through awareness and movement. Beautiful.
Ok, last question. To be crystal clear, internal work is not just for women, right? Men develop hypertonicity with the same frequency (if not more) than women and it’s a risk factor for not only pelvic pain but prostatitis, ya?
The pelvic floor and the obturator internus are easily accessed through the rectum. I see men in my practice as well. Prostatitis is usually the diagnosis they get from the urologist, when in fact, the painful symptom and urinary dysfunction is caused by the hypertonicity of the pelvic floor and other alignment factors.
YES! Fellas, don’t let your PF tension get out of control. It’s a major contributing factor to issues of the colon and prostate. This post is just as much for you as it is the ladies. (Hi Dad!)
Thanks for your time in answering my questions! If you’re in the SLC area of Utah, you’re lucky to have Susan as a potential therapist. Find more info about her practice, her classes, and her pregnancy/pelvic health workshops here: www.alignintegrationandmovement.com
Now let’s say for a moment that someone with a pelvic floor issue just can’t bring themselves to sign up for internal work yet. Susan and I have each come up with a few tips that can help with habits that create or perpetuate hypertonus. I’ll post those in the next day or so, because this post is too long already!